Data sources
Hospitalization and ED visit data are collected by the Canadian Institute for Health Information (CIHI) on a fiscal year basis. For hospital visits, the main diagnostic code is the “most responsible diagnosis” (MRD) that is deemed to be the clinically significant reason for the visit. For ED visits, the main diagnostic code is the “main problem” (MP). Hospitalization and ED visit data provide only a crude measure of the burden of cannabis use. Data are influenced by factors that are unrelated to health status such as availability and accessibility of care, administrative policies and hospital procedures. This may influence comparisons between areas and over time.
For all indicators, data were analyzed by the residence of the patient, not where the hospitalization or ED visit occurred. Ontario residents treated outside of the province were excluded. Data were reported by calendar year, based on the year of the hospitalization or ED visit. This report includes hospitalization and ED visit indicators with relevance to public health programming.
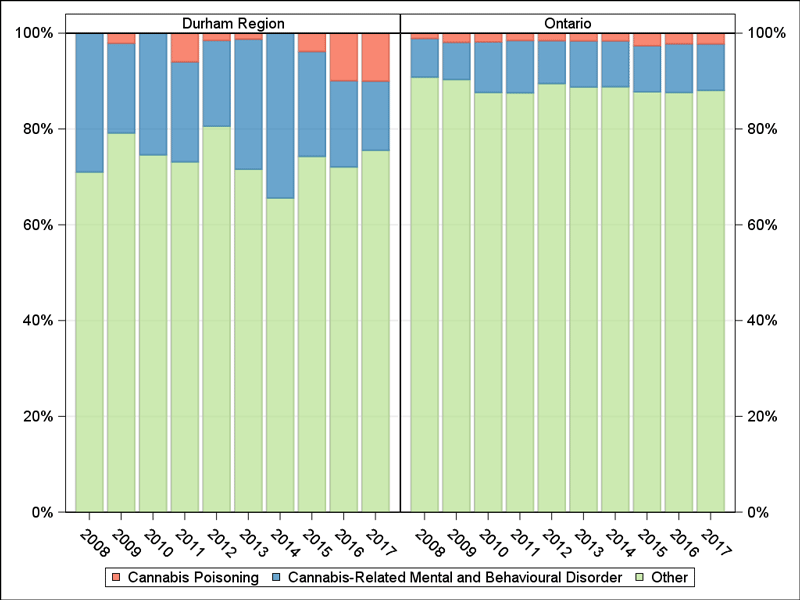
Cannabis-related hospitalizations and ED visits were selected using ICD-10-CA codes T40 (.7) (i.e., poisoning) and F12 (.0-.9) (i.e., mental and behavioural disorders due to acute intoxication, harmful use, dependence, etc. from the use of cannabinoids) whether it was the MRD/MP or comorbidity. This excludes injuries such as from motor vehicle traffic crashes or chronic conditions such as cancer where cannabis may be a contributing factor. Hospitalizations to designated adult mental health hospital beds were not included in this analysis. ED visits where the health care provider documented uncertainty in the diagnosis (diagnosis prefix Q) and ED visits that resulted in a transfer to another ambulatory care facility were included in the counts. Hospitalization and ED visits for mental and behavioural disorders due to multiple drug use (F19) were excluded. Multiple codes can exist for each hospitalization or ED visit. As such, a unique visit number, DAD key (hospitalizations) or NACRS key (ED visits), was used to count the number of hospitalizations or visits where at least one of the above codes was captured as the MRD/MP or comorbidity. In Figure 5, there is no distinction between prescription and illegal cannabis use.
Definitions
Figures and tables are provided for the following indicators:
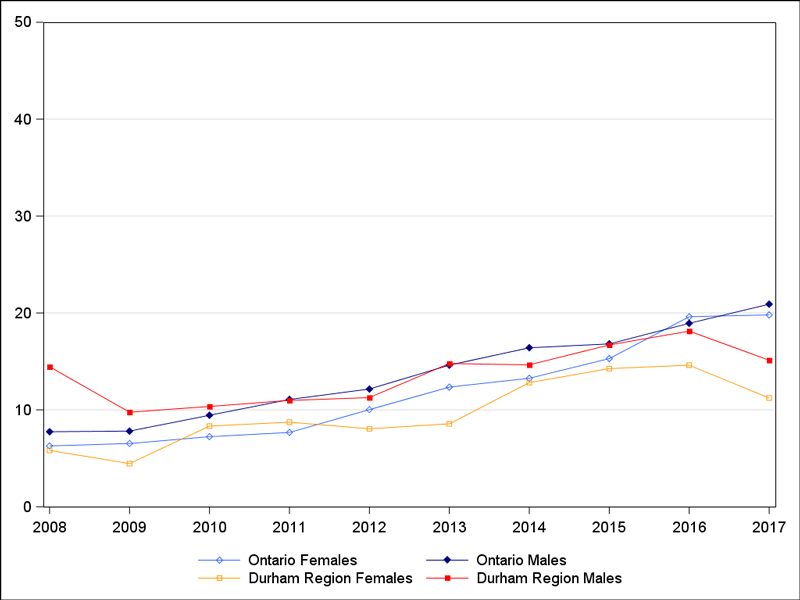
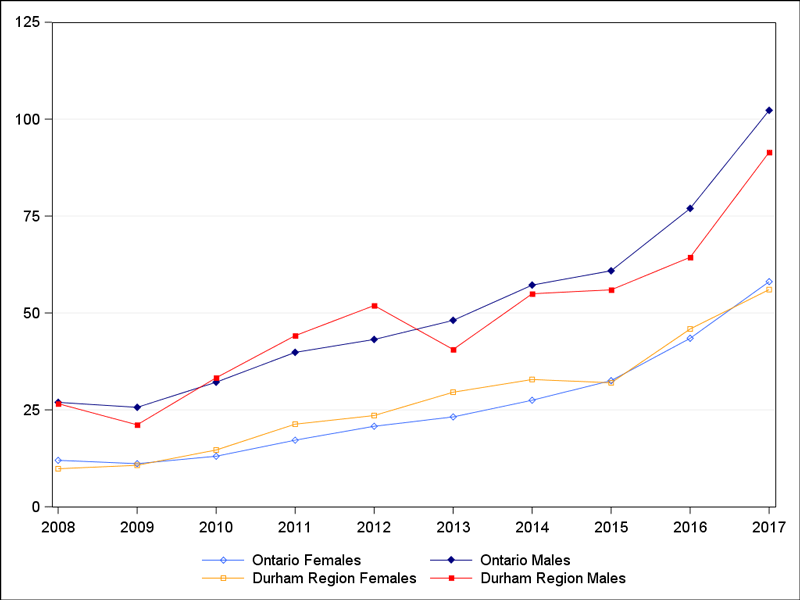
- Age-standardized cannabis-related Hospitalization and ED visit rates by sex
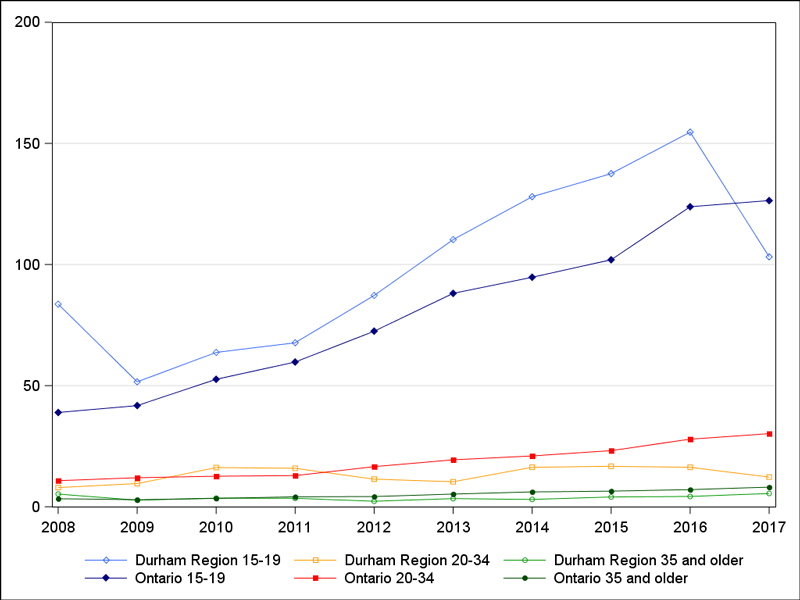
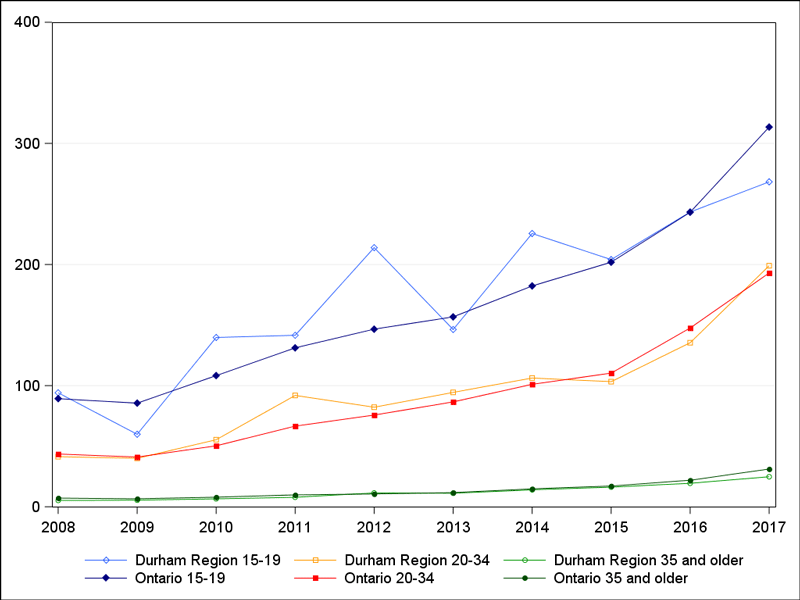
- Age-specific cannabis-related Hospitalization and ED visits rates in individuals aged 15 to 19 years, 20 to 34 years and 35 years and older
Age-standardized Hospitalization/ED visit rate
An age-standardized Hospitalization/ED visit rate is the number of Hospitalization/ED visits per 100,000 that would occur if the population had the same age distribution as the 2011 Canadian population. This rate provides a single summary number that allows populations with different age compositions to be compared.
Age-specific Hospitalization/ ED visit rate
This rate is the total number of Hospitalizations/ED visits in a specified age group per 100,000 population in that age group. The numerator and denominator refer to the same age group.